How the calf squeeze test works, what a positive result means, why it is the global standard for bedside Achilles rupture diagnosis — and what it cannot tell you.
In this article
When a clinician suspects an Achilles tendon rupture, the first thing they typically do is a simple physical test that takes about ten seconds and requires no equipment. They ask you to lie face down, let your feet hang off the end of the table, and then they squeeze your calf.
This is the Simmonds-Thompson test — often called the Thompson test, the calf squeeze test, or simply the squeeze test. It is the global clinical standard for initial diagnosis of Achilles tendon rupture, used in emergency departments, GP clinics, and sports medicine settings worldwide. Understanding what it is testing, how it works, and what its limits are helps you make sense of your diagnosis.
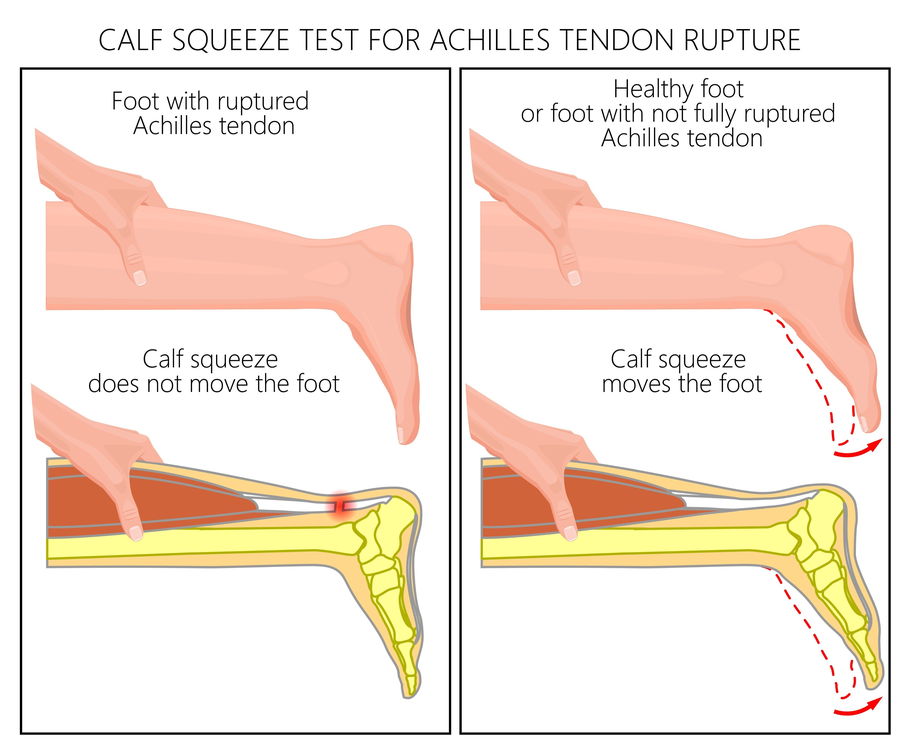
The Simmonds-Thompson test: squeezing the calf of an intact tendon causes the foot to plantarflex (move downward). When the Achilles is ruptured, the mechanical connection is lost and the foot does not move.
- A Brief History
- How the Test Works
- How Accurate Is It?
- What the Test Cannot Tell You
- Why Is It Called Both Names?
- What Happens After a Positive Test?
A Brief History
The test is named after two clinicians who described it independently. Franklin Simmonds, a British orthopaedic surgeon, first described the calf squeeze test in 1957 in a short paper in The Practitioner. Thomas Campbell Thompson described the same test independently in 1962 in Acta Orthopaedica Scandinavica, and subsequently published further work refining its interpretation.
The name "Thompson test" became more widely used in North America, while "Simmonds test" remained more common in the United Kingdom and Australia — hence the combined attribution "Simmonds-Thompson," which more accurately credits both clinicians. The Journal of Foot and Ankle Surgery noted in 2016 that referring to it simply as the "Thompson test" is technically incorrect, and that Simmonds' earlier description should be acknowledged.
How the Test Works
The test exploits the mechanical relationship between the calf muscle complex and the foot. Under normal conditions, the gastrocnemius and soleus muscles connect to the heel bone (calcaneus) via the Achilles tendon. When the calf is compressed, the muscle bellies are squeezed, which normally transmits force through the tendon and causes the foot to plantarflex — to point downward.
When the Achilles tendon is completely ruptured, this mechanical link is broken. Compressing the calf still creates muscle movement, but the force has nowhere to transmit — the foot does not move. This absence of movement is the positive result that indicates rupture.
1
Patient Position
The patient lies prone (face down) on an examination table with both feet hanging unsupported off the edge — or kneeling on a chair or stool. This position removes active muscle contribution and gravity from the result.
2
Calf Compression
The clinician firmly compresses the midpoint of the calf — the muscular bulk of the lower leg, not the tendon or heel. A firm, adequate squeeze is required; an insufficient squeeze can produce a false negative result.
3
Observation of Foot Movement
The clinician observes whether the foot moves downward (plantarflexes) in response to the compression. Both feet are typically tested for comparison — the uninjured side first to establish a baseline.
4
Interpretation
The presence or absence of foot movement is interpreted alongside other findings — the patient's history, palpation of the tendon, and any visible or palpable gap. The test result alone does not constitute a complete diagnosis.
Negative — Tendon Likely Intact
The foot plantarflexes (moves downward) when the calf is compressed. This indicates an intact mechanical connection between the calf and the heel. A negative result does not exclude partial tears or other injury.
Positive — Rupture Indicated
The foot does not move, or moves minimally, when the calf is compressed. This indicates disruption of the tendon's continuity. A positive result is a significant clinical finding — imaging is typically ordered to confirm and guide treatment decisions.
How Accurate Is It?
The Simmonds-Thompson test is one of the most diagnostically accurate bedside clinical tests in musculoskeletal medicine for the specific condition it targets.
96–100%
Sensitivity for complete Achilles rupture (Maffulli, 1998; Wang meta-analysis, 2013)
93–100%
Specificity — ability to correctly identify those without rupture
#1
Most sensitive of all clinical tests for Achilles rupture — above palpation, Matles, O'Brien, and Copeland
A 13-year prospective study by Maffulli et al. (1998) compared five clinical tests for Achilles rupture diagnosis — palpation of the gap, the calf squeeze, the Matles test, the Copeland test, and the O'Brien test — across 202 patients. The calf squeeze test and the Matles test were significantly more sensitive than all others, with the calf squeeze achieving the highest sensitivity at 0.96. The authors concluded it should be the primary clinical screening test for Achilles rupture.
"The calf squeeze test and the Matles test were significantly more sensitive than the other tests. Both should be part of the standard clinical assessment for suspected Achilles tendon rupture." — Maffulli et al., 1998
What the Test Cannot Tell You
Despite its accuracy for complete ruptures, the Simmonds-Thompson test has important limitations that clinicians and patients should understand.
- It cannot reliably detect partial tears. Sensitivity drops to 38–84% for partial ruptures and as low as 12–46% for chronic injuries. A negative test does not exclude a significant partial tear.
- Accessory muscles can mask a rupture. The flexor digitorum longus, flexor hallucis longus, tibialis posterior, and peroneal muscles can all produce some degree of plantarflexion even when the Achilles is completely ruptured — producing a false negative result.
- Significant swelling can reduce accuracy. In the early post-injury period, haematoma and swelling around the tendon can obscure findings and allow residual movement that might suggest an intact tendon.
- Technique matters. An inadequate calf squeeze — particularly in patients with larger calf musculature — can produce a false negative. The test is operator-dependent.
- It cannot determine whether treatment should be surgical or conservative. Imaging — ultrasound or MRI — is required to assess the degree of tendon separation, which informs treatment decisions.
A Positive Test Is Not a Complete Diagnosis
A positive Simmonds-Thompson test is a strong indicator of complete Achilles rupture but does not replace imaging. Ultrasound or MRI is typically required before treatment decisions are made — to confirm the rupture, assess the degree of tendon gap, identify any associated injuries, and determine whether surgical repair is appropriate.
Why Is It Called Both Names?
The dual naming reflects a genuine historical ambiguity. Simmonds described the test in 1957; Thompson independently described essentially the same test in 1962 and 1962. Thompson's description became more widely cited in North American orthopaedic literature, while Simmonds' name was retained in British and Australian practice.
A 2009 paper in the Canadian Journal of Surgery by Douglas, Kelly, and Blachut specifically sought to "clarify" the Simmonds-Thompson test, noting that the positive result is when the foot fails to plantarflex — clarifying a point of occasional confusion where some practitioners misread a positive as foot movement rather than its absence.
What "Positive" Means
A positive Simmonds-Thompson test means the foot does not move when the calf is squeezed — indicating rupture. A negative test means the foot does move — indicating an intact tendon. The terminology follows standard diagnostic convention: positive = finding present (rupture indicated), negative = finding absent.
What Happens After a Positive Test?
A positive Simmonds-Thompson test in the context of an appropriate clinical history — sudden calf pain, the sensation of being struck from behind, an audible pop — is considered a strong presumptive diagnosis of complete Achilles tendon rupture. From here, the typical pathway includes:
- Immobilisation of the foot in plantarflexion — either via splint, cast, or walking boot — to protect the tendon ends
- Imaging confirmation — usually ultrasound, which can be performed rapidly in most emergency or orthopaedic settings, and MRI in cases of uncertainty or operative planning
- Referral to an orthopaedic surgeon or sports medicine physician to discuss treatment — operative versus non-operative management
- Commencement of the recovery pathway — whether surgical or conservative — which typically involves a graduated weight-bearing protocol in a walking boot
If You Are Reading This Because It Just Happened
If you have had a positive Simmonds-Thompson test and are trying to understand what comes next — the diagnosis page covers the full picture of what to expect, and the recovery timeline outlines what the coming months look like. You are not alone in this.
References
1. Simmonds FA. The diagnosis of the ruptured Achilles tendon. Practitioner. 1957;179:56–58.
2. Thompson TC. A test for rupture of the tendo achillis. Acta Orthop Scand. 1962;32:461–465.
3. Thompson TC, Doherty JH. Spontaneous rupture of tendon of Achilles: a new clinical diagnostic test. J Trauma. 1962;2:126–129.
4. Maffulli N. The clinical diagnosis of subcutaneous tear of the Achilles tendon: a prospective study in 174 patients. Am J Sports Med. 1998;26(2):266–270. PubMed PMID: 9548124.
5. Wang D et al. Diagnostic accuracy of the Thompson test for acute Achilles tendon rupture: a systematic review and meta-analysis. Injury. 2013;44(6):769–775.
6. Douglas J, Kelly M, Blachut P. Clarification of the Simmonds-Thompson test for rupture of an Achilles tendon. Can J Surg. 2009;52(3):E40–E41. PMC2689757.
7. Garras DN et al. Are You Positive That the Simmonds-Thompson Test Is Negative? A Historical and Biographical Review. J Foot Ankle Surg. 2016;55(4):871–875.
8. Grokipedia. Thompson test — diagnostic accuracy and limitations. January 2026.
General health information only. This article is not medical advice. If you suspect an Achilles tendon rupture, seek urgent medical assessment. The Simmonds-Thompson test must be performed by a qualified clinician — it cannot be reliably self-administered.
Related
Full Diagnosis Guide →
→