Understanding the injury
The Achilles tendon
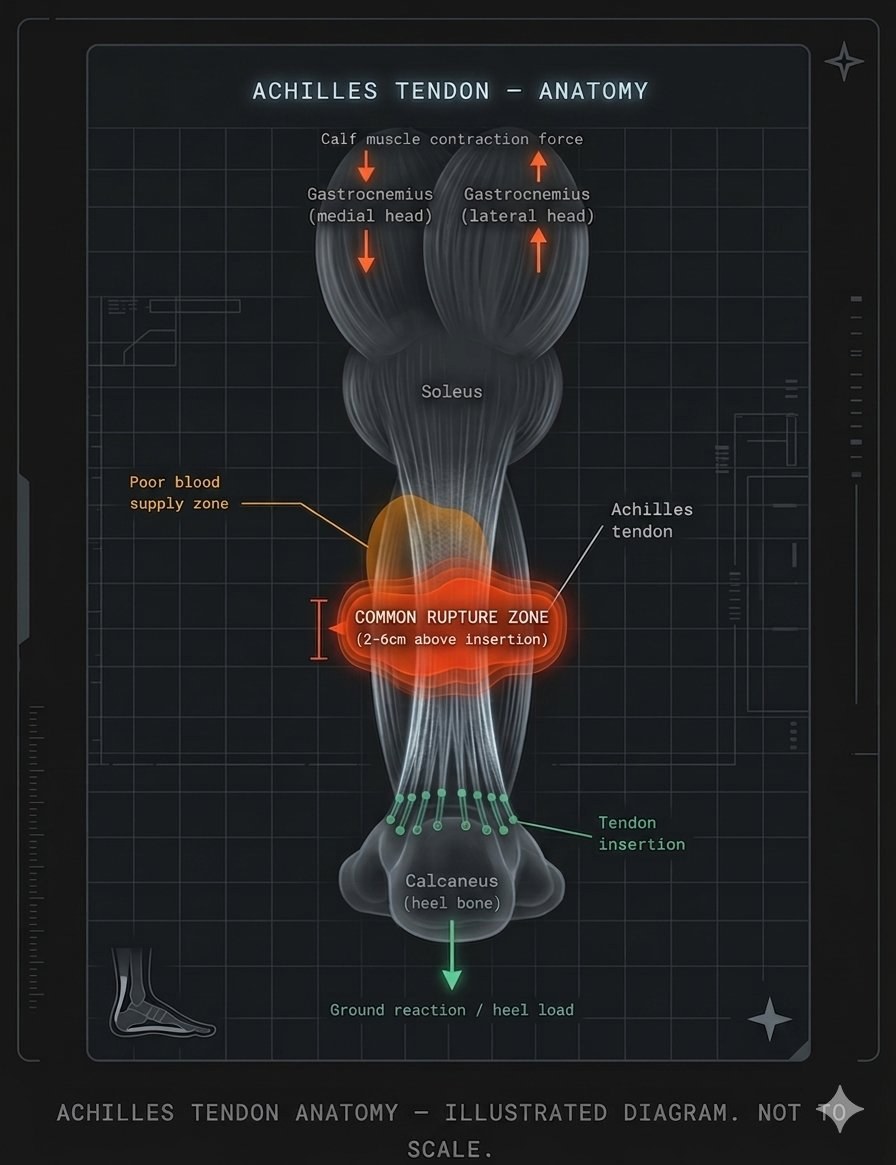
The Achilles tendon is the strongest and largest tendon in the human body. It connects the gastrocnemius and soleus calf muscles to the calcaneus (heel bone), and is responsible for plantarflexion — the movement that powers walking, running, and jumping.
Ruptures most commonly occur 2–6cm above the heel insertion point, in a zone of relatively poor blood supply. This is why healing is slow and why the early weeks of immobilization are critical.
The Achilles tendon can withstand forces of up to 12.5 times body weight during running
Peak incidence of rupture is in men aged 30–50, typically during recreational sport
97% of ruptured tendons show signs of pre-existing degeneration at the time of rupture (Kannus & Józsa)
Rupture incidence has increased approximately 10-fold over the past three decades